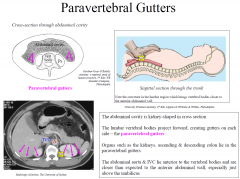
Left Paravertebral Gutter

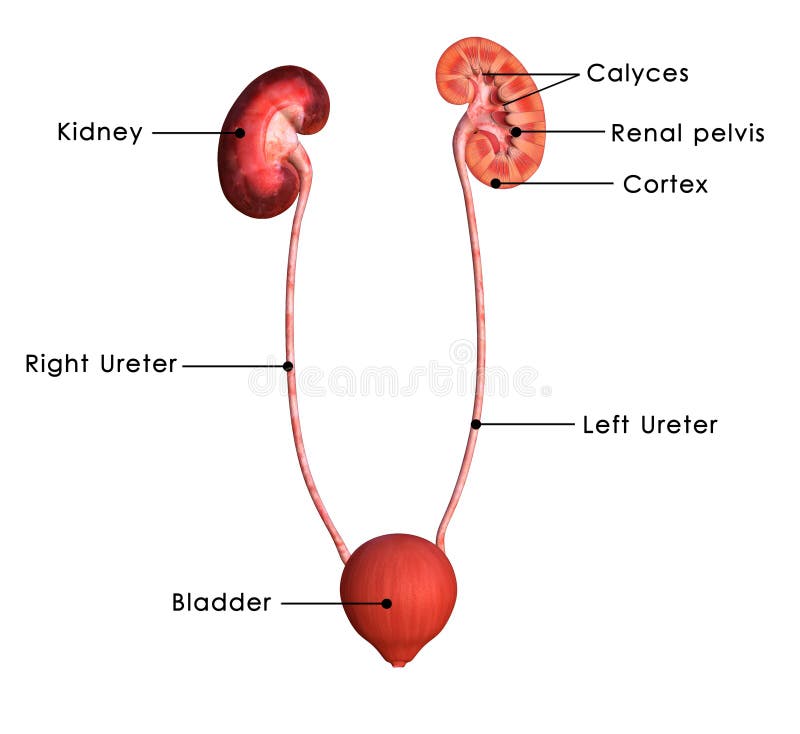
Urinary System Part 1 Flashcards Quizlet
Paravertebral Gutter Technique Diagram Radiology Case Radiopaedia Org
Paracolic Gutter
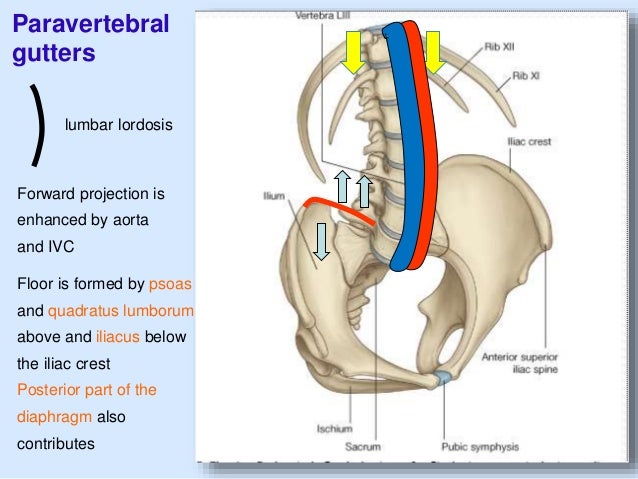
Posterior Abdominal Wall

Posterior Abdomen Flashcards Quizlet

Nb The Structures Psoas Major Muscle Lies In Paravertebral Gutter Between The Bodies And Transverse Processes Of The Lumb Vertebrae Anatomy Lumbar Puncture
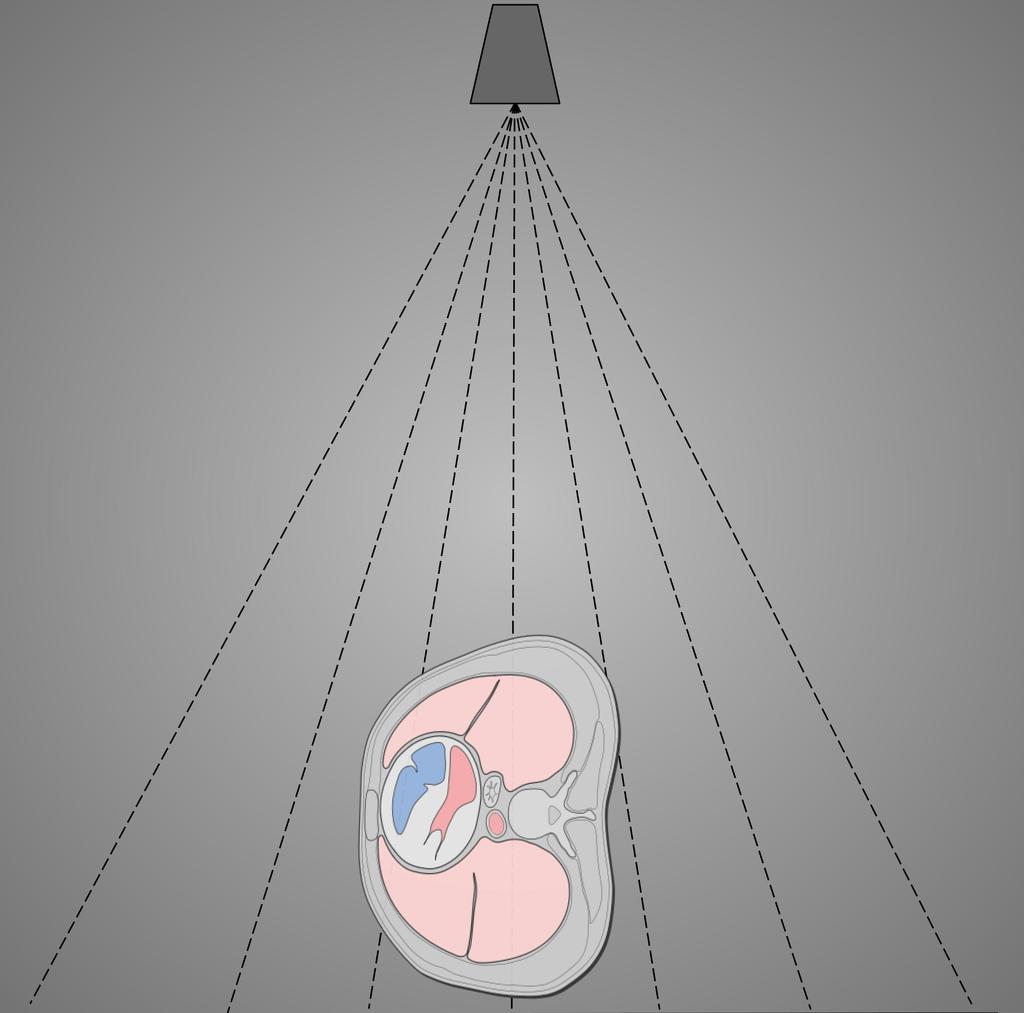
The midcoronal plane of the level of the 7 th thoracic vertebra approximately the inferior angle of the scapulae collimation.
Left paravertebral gutter.

Note Quadratus Lumborum Psoas Iliacus Muscle Iliac Crest Floor Of The Posterior Abdominal Wall Other Struct Plexus Products Spinal Nerve Muscle And Nerve
Paravertebral Gutter Stock Illustrations 33 Paravertebral Gutter Stock Illustrations Vectors Clipart Dreamstime

Posterior Abdominal Wall Last S Anatomy Regional And Applied

Lateral Chest Paravertebral Gutter Positioning Technique Wikiradiography
Posterior Abdominal Wall Flashcards Cram Com
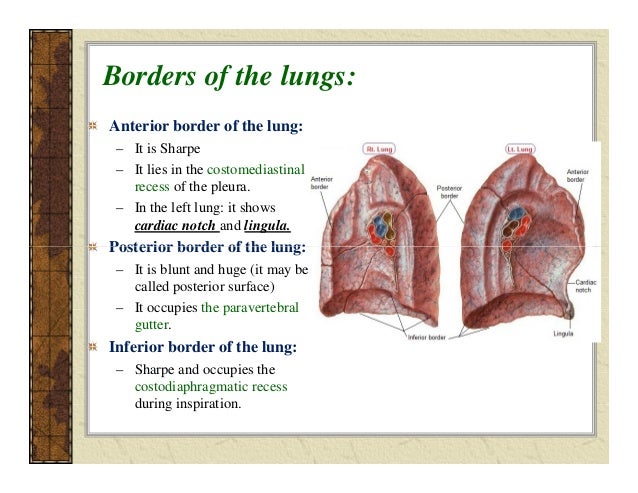
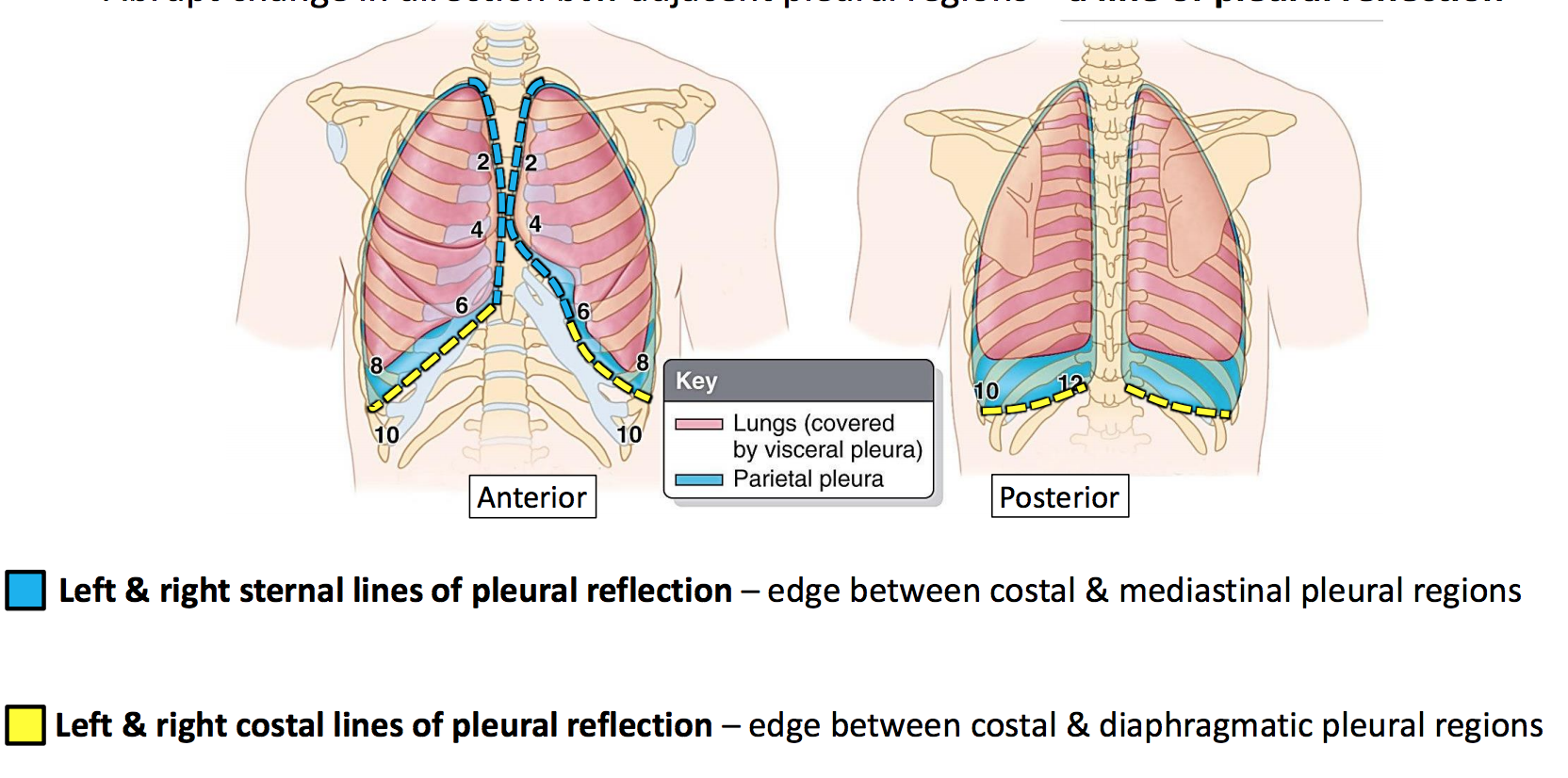
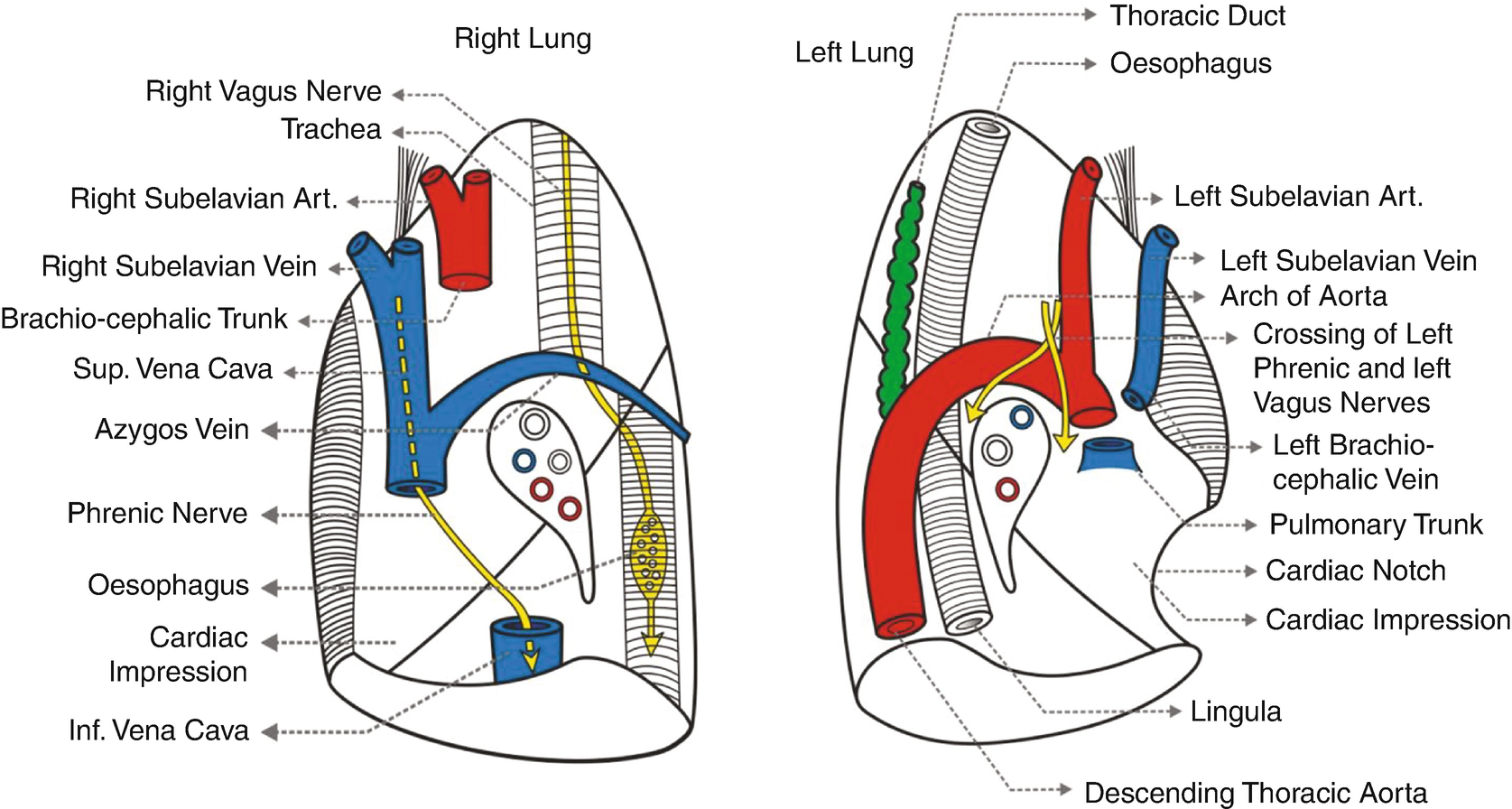
Https Www Studocu Com En Ie Document University College Dublin Clinical Human Anatomy I Lecture Notes Anatomy Of The Lungs Pleura 1974941 View
Lec 8 Lungs Pt Rc

Renal Anatomy Histology Correlate Ppt Video Online Download

3 A Huge Cyst In The Right Paravertebral Gutter Download Scientific Diagram

Marilyn Rose Kidneys Ureters Bladder Urethra Kidneys Retroperitoneal Bean Shaped Oblique Orientation Paravertebral Gutters Along Posterior Ppt Download
Anatomy Gs21 Lungs Pleura Updated Lordfred Adapted Flashcards Memorang

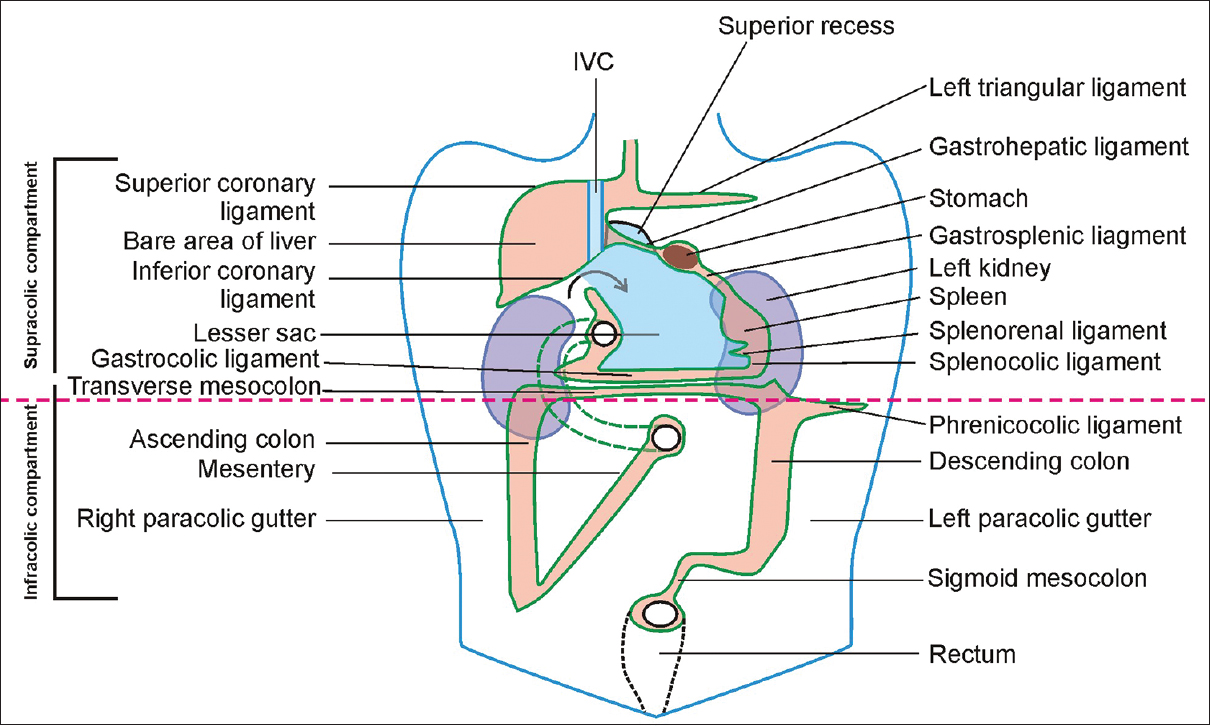
The Peritoneal Cavity Greater Sac Lesser Sac Teachmeanatomy

Renal Critical Care Northampton
Functional Anatomy Of Thorax Springerlink
Https Thorax Bmj Com Content Thoraxjnl 73 5 497 Dc1 Embed Inline Supplementary Material 1 Pdf Download True

Anatomy Of The Pancreas And Spleen Sciencedirect

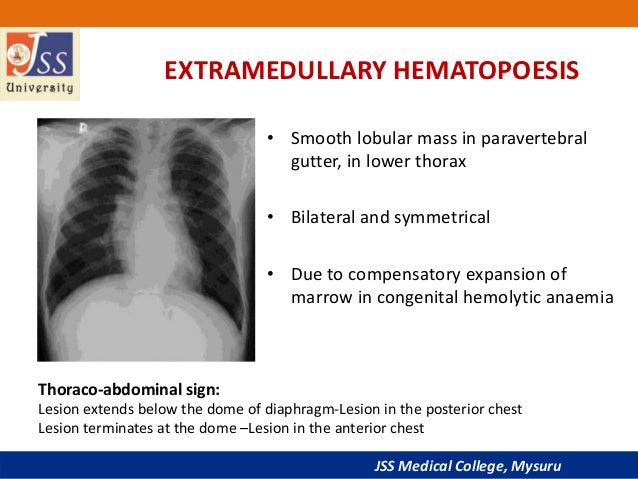
Chest Radiograph Showing Small Left Paravertebral Soft Tissue Mass Download Scientific Diagram

Kidneys
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcsmqktkaexvvbsqcnxolycoxthgnp6gciatuqeouumnwaizuz57 Usqp Cau

Anatomy Of The Thorax Thoracic Key

Systemic Venous Return Thoracic Key
Peritoneum Intraperitoneal Spaces
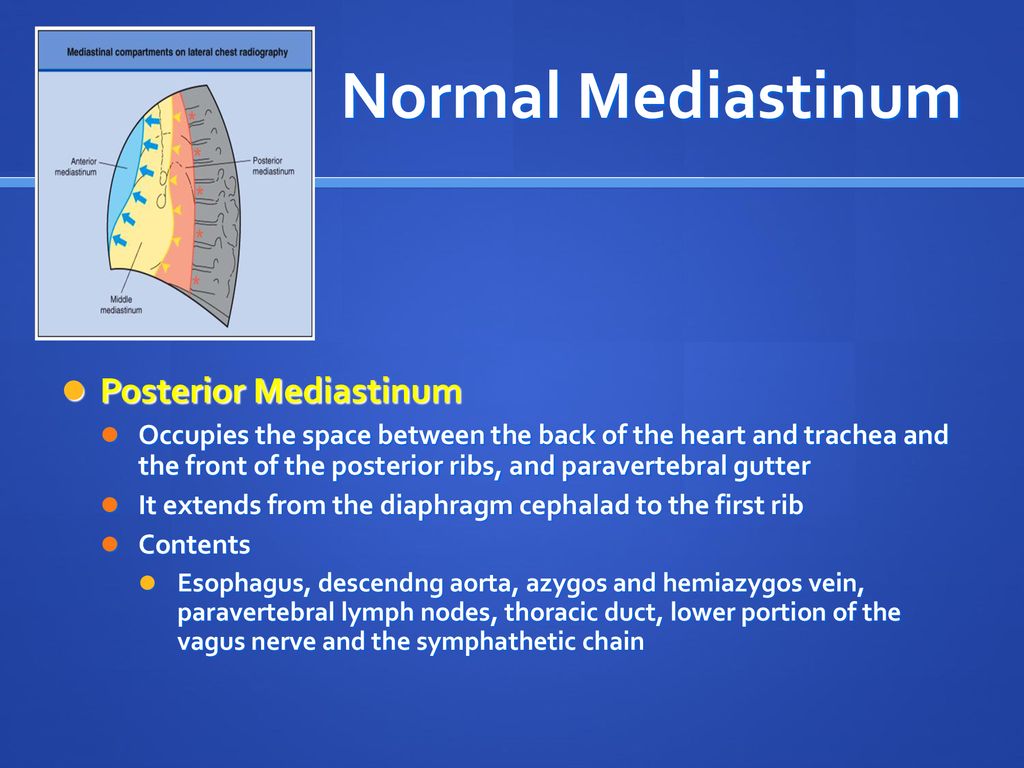
Introduction The Mediastinum Is The Region In The Chest Between The Pleural Cavities That Contain The Heart And Other Thoracic Viscera Except The Lungs Ppt Download
Chest X Ray Basic Interpretation
Source : pinterest.com
